Discover the essentials of chelating agents: their work, their key applications, and their role in detoxification and industrial processes.
Introduction:
Chelating agents ligands that can form two or more coordinate covalent bonds with a metal ion. One of the most common of these is 1, 2-diaminoethane. The molecules of the chelating agent create many connections with a metal ion and stop the metal from reacting properly. The core structure and chemical makeup of the metal ions are reorganized during the bonding process. Many metals have chemical structures that nearly resemble chains. These chain-like structures are joined at their ends by the chelating agents to create a stable ring that can transit through various environments with ease.
Chelating agents are either natural or synthetic organic compounds, used for industrial, medical, and biological applications. They help in the digestion processes, both in humans and animals, and transport nutrients in plants.
In medicine, chelating agents are used to remove toxic metals from the body. Mercury, arsenic, and lead poisoning can be treated with chelation therapy. Chelating agents change these metal ions into an excretable state that is chemically and biochemically. Specific chelating agents bind iron, lead, or copper in the blood and can be used to treat excessively high levels of these metals.
The ligands (electron donors) used in the chelation process are known as chelates, chelators, chelating agents, and sequestering agents.
Characteristics Of Ideal Chaleting Agents:
- Greater Affinity, low toxicity
- Ability to compete with natural Chelating Agents
- Ability to penetrate cell membranes.
- Rapid elimination of the toxic metal.
- High water solubility
- Capacity to form nontoxic complexes
- Same distribution as the metal.
Chelating Agent Compound Uses:
In Wilson’s disease patients on maintenance therapy, zinc is utilized to stop the absorption of copper.
In order to provide nutritional supplements, chelation is helpful. Chelation therapy uses it to get rid of harmful metals from the body. In MRI scanning, chelate compounds are utilized as contrast agents. The production of homogeneous catalysts uses these substances. Plants use the chelation process to get rid of heavy metals.
Chelating Agents Used A Drug:
- Dimercaprol
- Dimercaptosuccinic acid
- Disodium edetate
- Calcium disodium edetate
- Pencillamine
- Desferrioxamine
- Deferiprone
Chelating Agent And Their Role In Poisoning:
- Wilson’s disease is an inherited disorder in which there is too much copper in the body’s tissues. The excess copper damages the liver and nervous system. The medication used Trientine is a chelating agent. A chelating agent works by removing a heavy metal (such as lead, mercury, or copper) from the blood.
- Iron overload is the accumulation of iron in the body from any cause and the medication used (Exjade) is a Chelating Agents used to treat chronic iron overload syndrome caused by a genetic blood disorder (non-transfusion-dependent thalassemia) in adults and children.
- Lead is a toxic metal that affects the nervous system. It is absorbed primarily through the inhalation of lead dust and ingestion of lead products. Severe lead poisoning may be accompanied by hearing problems, headaches, nausea and vomiting, abdominal pain, loss of appetite, constipation, muscle soreness, anemia, and neurologic impairments such as stumbling or loss of concentration, and seizures. Medication used Succimer is a chelating agent that binds to lead in the blood and allows it to be passed out in the urine.
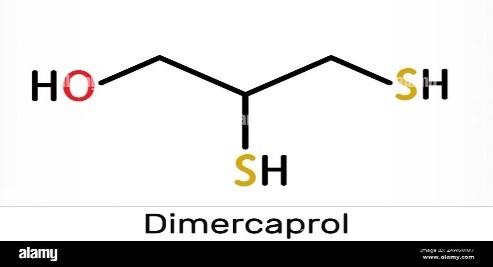
Dimercaprol:
Brand name or other name: BAL (British anti-lewisite)
Class Of drug: Chelating Agents
Structure:
Introduction:
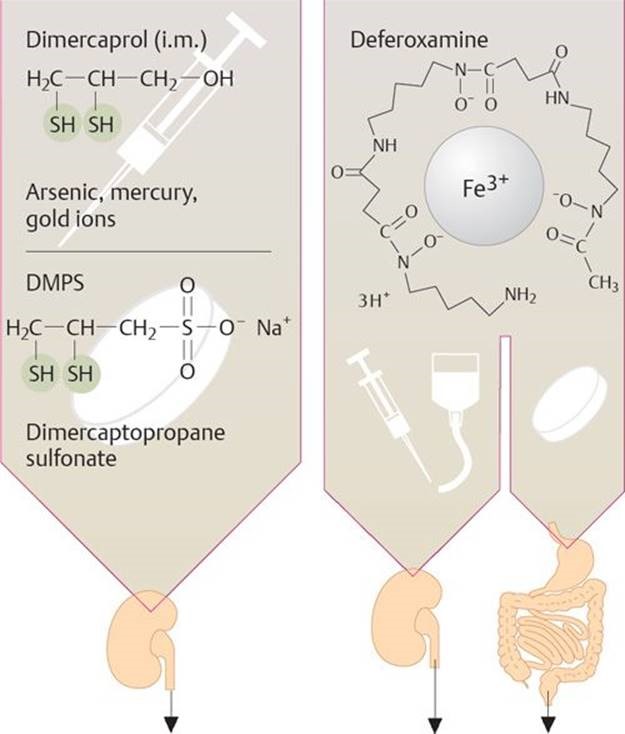
Dimercaprol is a drug that is used as an antidote to treat the poisoning of arsenic, mercury, gold, and acute lead poisoning with the combination. It is also used to treat Wilson’s disease in some rare cases of Chelating Agents.
Background:
Dimercaprol is a conventional chelating agent advanced by British biochemists at Oxford University at some point in World War II. It changed into advanced as an experimental antidote in opposition to the arsenic-based totally poison fuel Lewisite. It has been used clinically due to the fact 1949 in arsenic, cadmium, and mercury poisoning. In addition, it has in beyond been used for the treatment of Wilson’s disorder, a genetic sickness in which the frame tends to maintain copper. Dimercaprol has a poisonous ability, and its use may be accompanied by plenty of unfavorable results.
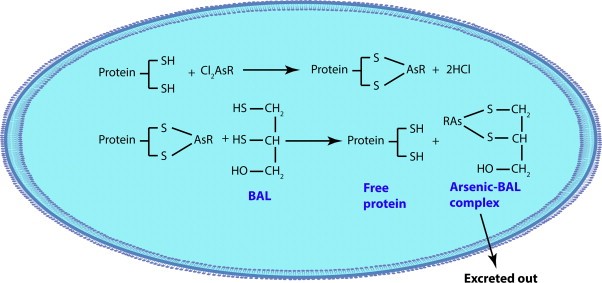
Mechanism Of Action:
The sulfhydryl groups of dimercaprol form complexes with positive heavy metals accordingly stopping or reversing the metallic binding of sulfhydryl-containing enzymes. The complication is excreted within the urine.
Dimercaprol has –SH organizations in its structure and competes with the thiol groups of enzymes for binding with arsenic or different metals to shape a strong metallic–chelate complex. The formed complex is then excreted from the body via urine. BAL forms heterocyclic ring complexes with metals.
The metabolism of dimercaprol of Chelating Agents has not been properly defined however it is hastily metabolized to inactive products including glucuronide conjugate. If the dimercaprol metal complex is oxidized the metal is launched and exerts its poisonous consequences.
Thus, the dosage of dimercaprol needs to be excessive enough to guarantee the extra loose dimercaprol to be had in body fluids until the metal is excreted.
Therapeutic Indication of Dimercaprol:
- Dimercaprol correctly chelates radioactive and solid nuclides of mercury, lead, arsenic, gold, and polonium-210.
- Dimercaprol is an FDA-accepted treatment for arsenic, gold, and mercury poisoning. It is also used in acute lead poisoning when used concomitantly with EDTA.
- Dimercaprol is effective for use in acute poisoning using mercury salts if the remedy is started within 1 to 2 hours following ingestion.
- Dimercaprol is of unknown amount in poisoning resulting from other heavy metals which include antimony or bismuth.
Dosing:
- Heavy metal poisoning: IM Adult
1st day: 400-800 mg
2nd day: 200-400 mg
3rd day: 100-200 mg
- Lead Poisoning: Initial 4 mg/kg (75-83 mg/sq. meter) IM, Repeat dose at least 4 hours later (but not until adequate urine flow established), THEN4 mg/kg (75-83 mg/sq. meter) + EDTA 250 mg/sq. meter IM every 4 hours for 3-5 days
- Wilson Disease: Not commonly used because of deep IM injection of 2-3 mL that is painful,2.5-3 mg/kg IM Bid/three times daily
Storage: It should be stored between 20-25O
Chemical Properties:
Dimercaprol is a straightforward propranol molecule with two sulfhydryl groups that binds heavy metals and competes with and blocks the binding of the harmful metals to enzymes in the body that contain sulfhydryl groups. BAL’s molecular weight is 124.21 and its empirical formula is C6H8OS2. It has a short half-life and is an oily, transparent, colorless liquid with the pungent, disagreeable smell associated with mercaptans.
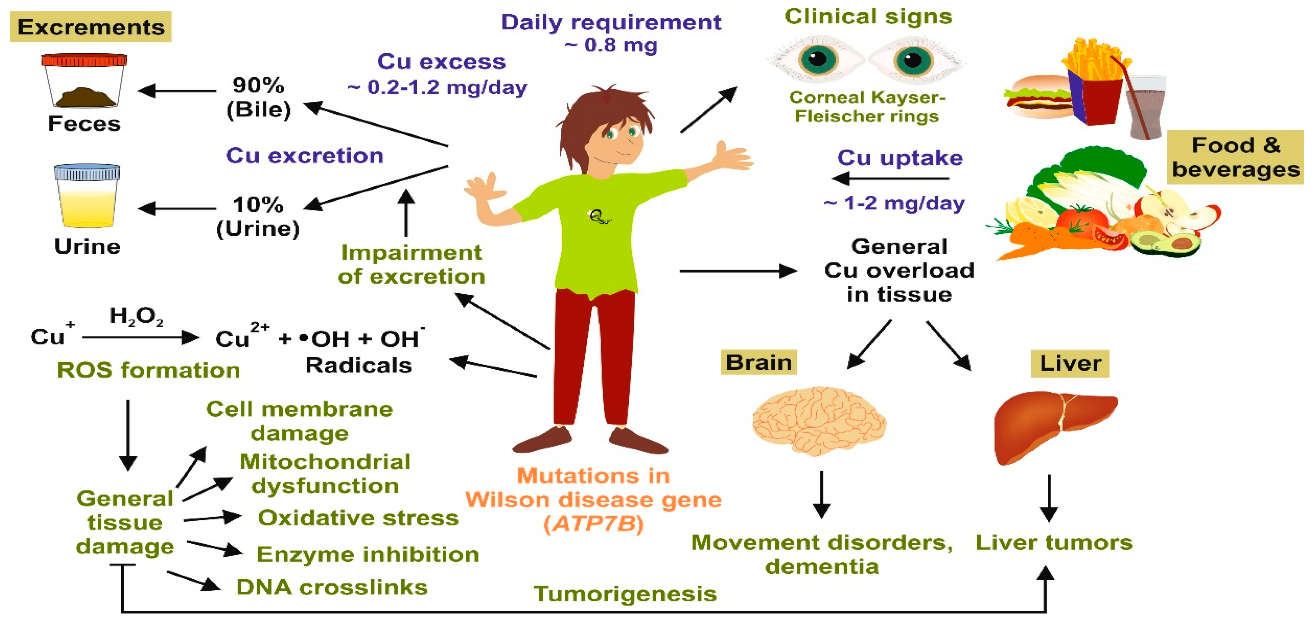
Wilson’s Disease:
Wilson disease is a genetic condition in which the body develops excessive copper buildup, mainly in the liver, brain, and eyes. The initial signs and symptoms of Wilson’s illness often develop between the ages of 6 and 45, but they typically start in adolescence. The characteristics of this syndrome combine liver disease with neurological and mental issues.
When a patient is identified with Wilson disease later in life, they normally do not exhibit any liver-related symptoms, however, they may have very minor liver disease. Liver disease is typically the first indication of Wilson disease in affected children and young adults.
Pharmacokinetics:
Absorption: After a deep intramuscular injection, dimercaprol undergoes fast absorption. Within 30 to 60 minutes, the plasma concentration reaches its maximum.
Distribution: Due to its high lipophilicity, dimercaprol easily enters the intracellular region. As a result, it is spread throughout all tissues, with the liver, kidneys, brain, and small intestines having the highest concentrations.
Metabolism: Without a metal complex, dimercaprol is metabolized by the liver by glucuronidation and into inactive metabolites.
Excretion: Dimercaprol has a brief half-life and is either complexed with metal or eliminated as an inactive metabolite. Dimercaprol is primarily excreted by the kidneys, but some is also passed through the bile. Metal can be redistributed into renal tissue as a result of the dissociation of the metal and sulfhydryl group’s link in acidic tubular urine. The plasma dimercaprol concentration must be kept at a level that promotes the ongoing synthesis and excretion of the stable dimercaprol-metal complex.
Side Effects:
If you have any of the following symptoms of an allergic reaction, get emergency medical attention right away: hives; trouble breathing; and swelling of your face, lips, tongue, or neck.
Although side effects are quite common, at the therapeutic dosage used, they are virtually always treatable and rarely severe enough to require stopping treatment. A little amount of research suggests that taking 30–60 mg of ephedrine sulfate orally 30–60 minutes before each injection of dimercaprol will lessen adverse responses. A minimum time between doses of four hours also seems to lessen negative effects.
The following negative consequences of dimercaprol, especially at higher dosage levels:
- Abnormalities of the lymphatic and blood systems
- Additionally, hemolysis and a brief decrease in leukocyte count have been documented.
- Psychiatric disorders
- Anxiety
- Restlessness
- Nervous system disorders
- Tremor
- Headache
- Tingling in the hands and other extremities
- High doses have been linked to hypertensive encephalopathy,
- Coma and convulsions.
- Eye disorders
- Blepharospasm
- Lacrimation
- Conjunctivitis
- Eye-burning feeling
- Cardiac disorders
- A tachycardia-accompanied rise in blood pressure
- Diseases of the respiratory,
- Thoracic
- Mediastinum
- Rhinorrhoea is an uncomfortable tightness in the chest and throat
- Gastrointestinal disorders
- Stomach discomfort
- Salivation
- Nausea
- Vomiting
- Burning in the lips, mouth, and throat is also common.
- Hepatobiliary disorders
- Hepatotoxicity/liver injury
- Diseases of the skin and subcutaneous tissues
- The forehead and hands are perspiring
- Diseases of the muscles, bones, and connective tissues
- Jaw pain, spasms in the muscles
- Renal and urological conditions
- Renal dysfunction
- Breast and reproductive system problems
- The feeling of burning in the penis
- Conditions at the administration site and general problems
- The injection location may experience local pain, and gluteal abscess has occasionally been reported. Pyrexia.
- Investigations
- Blood zinc levels fell and the active partial thromboplastin time increased.
- Pediatric patients
- A fever that appears to be specific to children emerges after the second or third injection and lasts until dimercaprol medication is stopped.
Administration:
- The upper lateral region of the buttocks is where a deep intramuscular injection (IM) of dimercaprol is given.
- The injection sites alternate between the right and left buttocks, about two inches below the previous ones, over the course of many days to weeks.
- To safeguard renal function, it is also advised to maintain an alkaline urine pH.
- The main considerations for choosing dimercaprol therapy are blood and urine concentrations, symptom relief, and dimercaprol toxicity.
Contraindications:
- Any patient with a peanut allergy should not use dimercaprol because it is made with peanut oil. As soon as dimercaprol hit the market, peanut oil, which is lipid-soluble, became a popular product. Dimercaprol’s only alternative FDA-approved solvent is presently unavailable.
- In prolonged exposure to both inorganic and organic mercury, dimercaprol is regarded as contraindicated. According to Berlin and Rylander, animals getting dimercaprol treatment in combination with long-term exposure to organic mercury had mercury deposited in their brains as those receiving just mercury. DMSA is therefore the best chelating agent in these circumstances.
- Dimercaprol is contraindicated in liver deficiency. In animal experiments by Cameron et al., dimercaprol-treated mice and rabbits with hepatic impairment had toxic signs and eventually died. These effects took place in healthy animals at levels that were well below the fatal threshold. Due to a higher risk of hemolytic anemia in individuals with glucose 6-phosphate dehydrogenase impairment, dimercaprol therapy should be used with great caution.
Pregnancy And Lactation:
Pregnancy Class C:
Lactation:
Use caution during lactation since there is unknown excretion in milk.
Pregnancy Categories
Category A:
Acceptable generally. No fetal danger has been identified in controlled investigations of pregnant women.
Category B:
Possibly acceptable Animal studies either revealed minimal dangers and human studies were done and showed no risk, or animal studies showed no risk but human studies were not available.
Category C:
If advantages exceed hazards, proceed with care. Risk is demonstrated by animal research, but human studies are either not accessible or have not been conducted.
Category D:
When no safer medication is available, use it in LIFE-THREATENING situations. Evidence of fetal risk in humans.
Category X:
Avoid using if pregnant. The risks exceed any possible advantages. There are safer choices.
Toxicity:
- Rats’ intramuscular LD50 is around 105 mg/kg, whereas their intraperitoneal LD50 is 140 mg/kg. For mice, the intraperitoneal LD80 is around 125 mg/kg.
- In studies on animals, dimercaprol has been found to enhance the brain deposition of arsenite, organic mercury compounds, and the toxicity of cadmium and lead.
- In animal investigations, dimercaprol has been found to cause seizures and is nephrotoxic.
- Dimercaprol does not have an effective antidote. Therefore, it is advised to stop the medication until the symptoms go away if dimercaprol toxicity manifests.
- Dimercaprol medication should be continued, tapered down, or stopped as determined by clinical discretion.
Precautions:
· Due to the FORMATION OF TOXIC COMPLEXES, do not use with iron, cadmium, or selenium.
· For acute lead poisoning, combine CaNa-EDTA with additional medications.
· Oliguria, deficiency of G6PD· If renal failure develops, stop using this medication.